

Publications
INSS Insight No. 1303, April 21, 2020

The proposed strategies for exiting the coronavirus crisis have urged the continued isolation of at-risk population groups, including people aged 65-70 and older. The main argument raised is protection of “the elderly,” as the virus is particularly dangerous for this sector. Another argument addresses the threat to the healthcare system, should it be overloaded with elderly patients in serious condition. However, there are weighty considerations that counter the arguments for continued isolation of senior citizens. For the elderly who are not independent, isolation often leads to loneliness that has a proven negative impact on health. For the independent elderly, the ability to continue enjoying life is harmed by the fact that they are deprived of the ability to meet their friends and relatives or enjoy certain leisure activities. For seniors who are still employed, either as self-employed or as salaried workers, isolation may lead to forced retirement with the attendant economic impact and a loss of meaning to their lives, which also may damage their health. Imposed authoritarian restrictions constitute serious interference with the free will of the elderly. Those seniors who are of sound mind should be able to decide for themselves how much they want to expose themselves to the outside world, rather than suffering sweeping mandatory restrictions.
As part of the struggle against the spread of the coronavirus, all Israeli residents have been in some sort of lockdown, if not quarantine. The proposed exit strategies envision a gradual, multi-phased process that balances healthcare needs, i.e., containing the spread of the disease and maintaining the functionality of the health system, with economic needs, meaning reviving the economy and seeing a return to employment. One of the components of the plans dealing with the next stage is the continued confinement of “at-risk population groups,” including the elderly above a certain age, and those suffering from underlying chronic illnesses. Most proposals consider a person “elderly” – old enough to require him/her to remain in isolation – from the age of 65 or 70, although other ages are also mentioned, such as in one proposal relating to the opening of schools, which returns only teachers below the age of 50 to the classroom. This article relates to the entire “elderly” population affected by the restrictions.
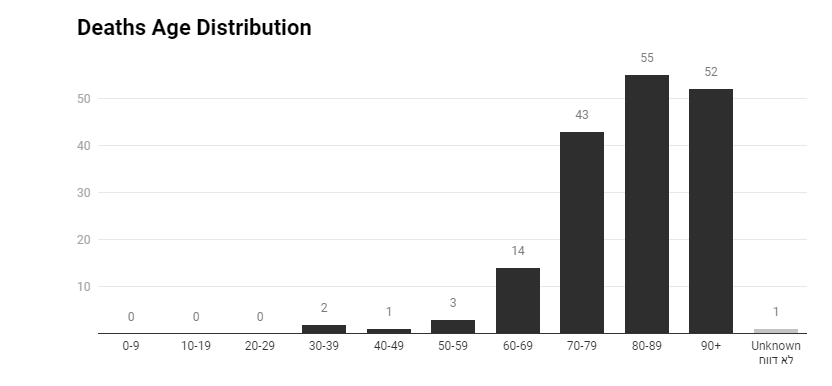
The main advantage of seniors remaining in isolation is in reducing their exposure to potential infection by the virus, which endangers them more than other age groups. According to data provided in the Gartner Institute Report that was presented to the government (Chapter 6 of the report), the risk of death from coronavirus is over 5 percent in the over-65 age bracket. According to Ministry of Health data, among those who have died from the disease in Israel, 3.6 percent are aged 60–70, 8 percent are aged 70–79, and 22 percent are above 80.
At the same time, there are significant costs for ongoing isolation, and these must be mapped. To do so, a distinction should be made between two population groups: seniors who have difficulty functioning independently, including those in nursing homes or confined to their homes, and independent seniors, which includes those who are still employed and active retirees.
From the standpoint of the former group, isolation often incurs more difficult living conditions, due to the lack of connection with family members and others who may have helped them prior to the pandemic. The isolation may also stem options for physical activity, including physiotherapy or light sport activities. Most of all, isolation intensifies solitude, and various studies have shown the extent to which solitude may lead to depression and inferior health. In other words, isolation in and of itself may have a negative impact and therefore the risk incurred with the isolation must be assessed and a proper response formulated.
From the standpoint of the second group, for whom solitude is relevant as well, particularly for those who live alone, isolation has additional significance. First, it bars any physical encounters between the seniors and family and friends, beyond those who live with them.
Second, it has a negative impact on the leisure culture of seniors, including physical activity, potential travel, shopping, dining out, or recreation. In other words, isolation may have a negative impact on the zest for life.
Third, isolation has a negative impact on the careers of seniors who cannot work from home. Leaving seniors in isolation while others are permitted to return to work raises the concern that they will lose their position even once this period is over, and in particular the more time elapses. Self-employed seniors may not be able to resume their businesses, and employees may find themselves leading the list of those dismissed in an age of cutbacks because they are in isolation. Their chances of finding new jobs are slim, which in turn entails serious economic implications. Beyond that, forced retirement has a negative impact on a person’s sense of self, and in the end, on his/her health. Studies show that people who continue at their jobs after retirement age experience fewer health problems such as high blood pressure, heart disease, diabetes, and depression.
The isolation of the senior population also has economic significance, whether direct, due to their contribution to the economy, as manufacturers and as consumers, or indirect, in that grandparents make a significant contribution to the ability of young parents, mainly mothers, to participate in the labor force.
Moreover, the isolation of senior citizens will have a negative impact on the country and its economy. Many senior positions in the private and public sector are held by people over the age of 65, including, for instance, Israel’s Prime Minister and President, as well as leading businesspeople. It is clear that it is unreasonable to prevent these officials and others in similar positions from continuing to serve. Therefore, inasmuch as part of the elderly population is exempted from the requirement of isolation, thorny questions of discrimination arise.
Insofar as the aim of the isolation is to shield the elderly themselves, the consideration may be overprotective, if not paternalistic, since the State is limiting their freedom "for their own good." For seniors who are “helpless,” i.e., those who realistically are unable to consider their own welfare, protective measures can be justified. Otherwise, imposing mandatory isolation constitutes serious intervention in their free will, especially when there are significant considerations against such isolation. Moreover, while isolation may reduce the risk of contracting the coronavirus, the risk of death from the disease is low, even for seniors, and particularly for those without underlying chronic illnesses.
Consequently, the decision as to their welfare rightfully belongs to the seniors. They should be allowed to decide whether to remain in isolation, without harming their rights – for instance, without their absence from work being considered unjustified. However, they must not be forced to remain in isolation only “for their good,” but must be allowed to decide for themselves.
Continued isolation of the elderly is also based on other considerations that relate to risks not to seniors but rather emanating from them. As for the risk that the elderly will contribute to the spread of the disease, as the Gartner Institute report explains, the representation of the elderly among the total number of those infected is lower than their relative share of the overall population, so isolating them will have a negligible effect on the scope of the spread of the disease. The main argument in this context is the protection of the healthcare system. It is argued that the infection of seniors leads to more cases of hospitalization and more cases needing intensive care and respirators. The concern is that this will lead to the collapse of the healthcare system, with a negative impact on the general public that requires its services. However, the scope of this concern needs fine-tuning. For example, the Gartner report determines that as long as various restrictions on normal routines on the general public are in place and there are a limited number of new cases, then even if the elderly patients require respirators, their treatment falls within the inclusion of the system. Indeed, the risk that healthy seniors will require respirators is not necessarily significantly higher than a younger population, In other words, the main risk refers to older people with underlying chronic conditions.
Moreover, while the concern of overloading the healthcare system is legitimate, it must be balanced with the damage that will be caused by continued isolation of the elderly. As part of creating this balance, instead of imposing sweeping restrictions on senior citizens, it is important to consider creative ways that allow for reducing the risk of infection on one hand, without causing serious damage to the quality of life on the other. There is room to allow seniors who are interested in remaining in isolation to do so, without harming their rights, and while providing a remote digital solution to their various needs. Those who are not interested in isolation should be allowed to leave while ensuring the conditions to reduce their risk of infection. For example, family gatherings can be held with up to a certain number of people instead of prohibited entirely. Conditions at work places can be created to reduce the concern of infection as much as possible. Designated hours can be set for seniors to shop at grocery stores and pharmacies, as has been implemented in many places abroad. Activity outside the house can be allowed for seniors with a restriction on the rest of the public, such as determining that in public parks, entry is permitted only to the elderly plus one accompanying person during certain hours.
It seems that this topic has not received sufficient attention in discussions on an exit strategy. It is crucial to have a special team to examine it and present detailed recommendations in conjunction with gerontology experts and representatives from the senior population.
The bottom line is that ongoing sweeping restrictions on senior citizens are not justified and will be difficult to enforce. Will police officers arrest seniors who contravene the directives? Rather, the proper way is to secure arrangements that balance the need to protect the healthcare system with the rights of the older population to exercise their free will and continue living lives with meaning and enjoyment. There is no place to make the last years of the lives of Israeli seniors miserable in the name of protecting their health.